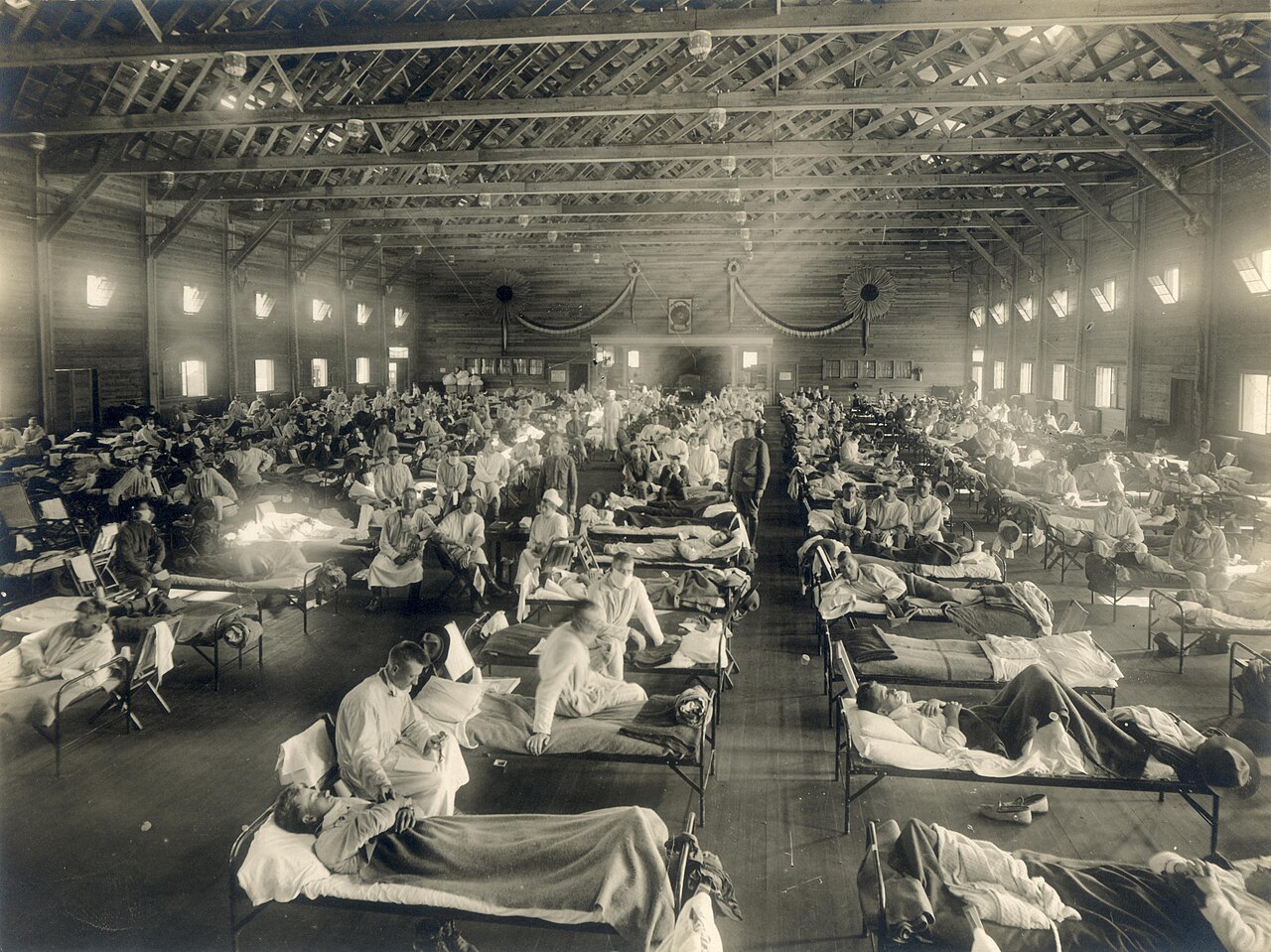
On the morning of 4 March 1918, Private Albert Gitchell walked into the hospital at Camp Funston, Kansas, complaining of a sore throat, fever, and headache. He was an Army cook — one of tens of thousands of young men passing through Fort Riley on their way to the trenches of France. The doctor noted his symptoms and sent him to bed. By noon, over a hundred soldiers had reported the same complaints. Within a week, five hundred were hospitalised. After five weeks, 1,127 men at Fort Riley had fallen ill and forty-six were dead. The familiar seasonal ailment — the flu, the thing you shrug off and go to work with — had become something else entirely.
Camp Funston was a processing centre. At its peak, it handled nearly 56,000 troops preparing for deployment to Europe. In March 1918 alone, 84,000 American soldiers sailed for France. In April, another 118,000 followed. They carried rifles, letters from home, and a virus that would kill more people than the war they were joining. The pandemic that began in a Kansas army hospital would circle the globe three times, infect a third of the world’s population, and leave somewhere between seventeen and fifty million dead — possibly as many as a hundred million, though the chaos of the era makes precise counting impossible. The First World War killed roughly twenty million. The flu that travelled with the armies killed at least twice that, and perhaps five times.
The outbreak probably did not start with Private Gitchell. A country doctor named Loring Miner had been reporting an unusually severe influenza in Haskell County, Kansas, since January 1918 — the first recorded notice of unusual flu activity anywhere in the world that year. Haskell County was farm country, and young men from those farms were already travelling to Camp Funston for training. The virus likely hitched a ride with them. From Funston it spread to other military camps, then onto troopships, then into the trenches, then into civilian populations across Europe, Asia, Africa, and back again. Wartime mobilisation did what no peacetime movement could have: it turned a local outbreak into a global catastrophe in a matter of months.
The pandemic was never Spanish. Spain was neutral in the war and had no press censorship. When the flu arrived, Spanish newspapers reported it freely — including the infection of King Alfonso XIII in May 1918. Meanwhile, Britain, France, Germany, and the United States were suppressing news of the outbreak to maintain wartime morale. Soldiers were dying of influenza in military hospitals, but the papers wrote about victory and sacrifice. The only country telling the truth about the disease was Spain, so the world assumed Spain was the source. The name stuck. It was a slander born of censorship, and the Spanish have been living with it for over a century.
The pandemic came in three waves. The first, in spring 1918, was relatively mild — high fever, aches, a few days in bed, then recovery. It resembled ordinary seasonal flu and killed at ordinary seasonal rates. The second wave, in autumn 1918, was the killer. The virus had mutated into something far more lethal. Healthy adults could wake with a cough in the morning and be dead by nightfall. Victims turned blue from lack of oxygen as their lungs filled with fluid. October 1918 was the deadliest month — in the United States alone, 195,000 people died of influenza that month. The third wave, in winter 1918–19, was less severe but still deadly, and the virus continued circulating for years afterward.
The death toll defied the usual patterns. Seasonal flu kills the very young and the very old — those whose immune systems are weakest. The 1918 flu killed young adults at rates that made no epidemiological sense. People aged twenty to forty died in disproportionate numbers. One theory is that their stronger immune systems overreacted to the virus, triggering a cytokine storm that destroyed their own lung tissue. Another is that older people had some residual immunity from a similar strain that had circulated decades earlier. Whatever the cause, the pandemic hollowed out a generation. It killed more American soldiers than German artillery.
The public health response included something that would become grimly familiar a century later: mask mandates. San Francisco enacted a mask ordinance on 25 October 1918, requiring face coverings in public. The Red Cross sold masks at ferry terminals. Newspapers published sewing instructions. Compliance was initially high — around eighty per cent — and the city’s health officer declared the measure a success. Violators faced fines and jail time. The mayor himself, James Rolph, was caught maskless at a boxing match and fined five dollars.
The ordinance lasted less than a month. By late November, with cases falling, the city lifted the requirement. When infections surged again in December, a second mandate took effect in January 1919. This time, the resistance was organised. The Anti-Mask League of San Francisco held a public meeting on 25 January 1919, drawing 4,500 citizens to protest the requirement. The league’s members included physicians, civil libertarians, and at least one member of the Board of Supervisors. They argued that masks were ineffective, that the mandate violated personal liberty, that the science was uncertain. Some wore their masks with holes cut for cigarettes. The arguments were identical to those heard in 2020, down to the phrasing. The league’s president was a suffragist and attorney named Emma Maria Harrington. The mask mandate was repealed within weeks. San Francisco’s death rate from the pandemic was among the highest of any American city.
The Spanish flu is one of the few pandemics that the general public remembers. Before COVID-19, it was probably the only one most people could name, let alone date. The Black Death is a phrase from history class; cholera and typhus are diseases of the past; even the 1957 and 1968 flu pandemics have faded from collective memory. But the 1918 flu left a mark deep enough to persist — in family stories, in the empty chairs at tables, in the mass graves that cities dug when the coffin-makers could not keep up.
I think about this when I hear people dismiss the seasonal flu as a minor inconvenience. In most years, it is. Influenza kills tens of thousands annually, but the deaths are spread thin enough that we absorb them without alarm. We skip the vaccine because we are busy, or sceptical, or convinced that the flu is something that happens to other people. And usually we are right. The virus circulates, some people get sick, most recover, and life continues. But influenza is not a solved problem. It mutates constantly. Every few decades, a strain emerges that our immune systems do not recognise, and the familiar killer shows what it can do when the conditions align.
On 4 March 1918, a cook with a sore throat walked into a Kansas hospital, and the world changed. The war that followed the pandemic reshaped borders and toppled empires, but the virus killed more people than the bullets did. A century later, we have better medicine, better surveillance, better vaccines — and the same arguments about masks, the same resistance to public health measures, the same confidence that it will not happen here, not to us, not this time. The 1918 flu is a warning written in tens of millions of deaths. Whether we read it is another matter.